The Pediatric Advanced Life Support (PALS) Precourse Self-Assessment is an online tool that evaluates a student’s knowledge before the PALS Course to determine their proficiency and identify any need for additional review and practice.
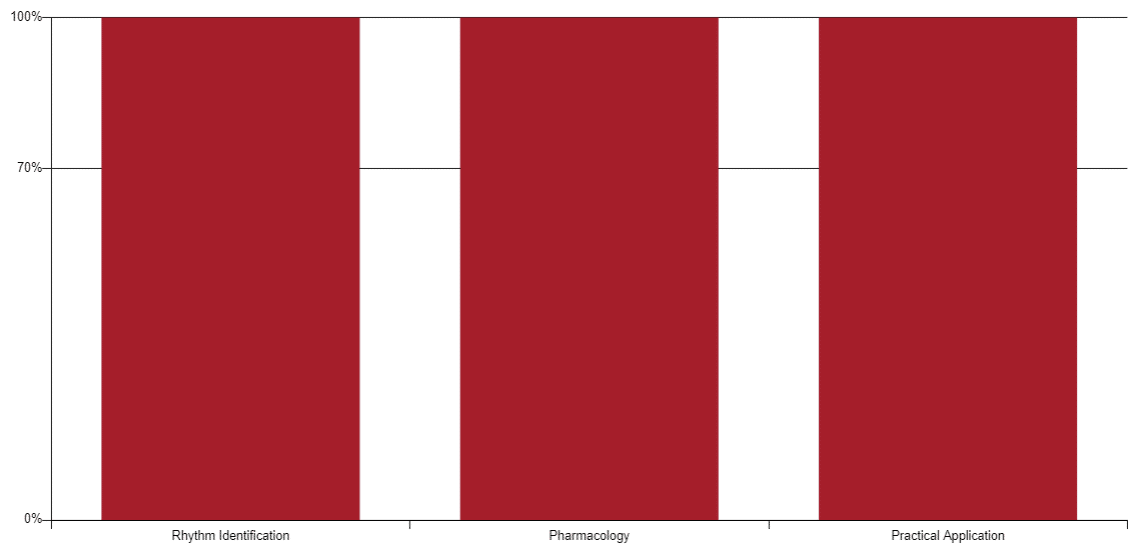
This assessment consists of 52 multiple-choice questions in rhythm identification, pharmacology, and practical application, taking about 1 to 1½ hours to complete. A 70% or higher score is required to pass, and students must print their scoring report and bring it to class.
This page provides key information about the PALS Precourse Self-Assessment and free answers to it.
PALS Precourse Self-Assessment Answers 2023
Section 1: Rhythm Identification Answers
For section 1, identify the rhythm by selecting the single best answer.
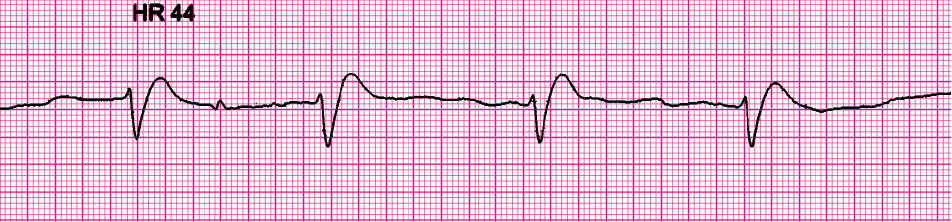
Clinical clues: heart rate 44/min; no detectable pulses.
Answer: Pulseless electrical activity.
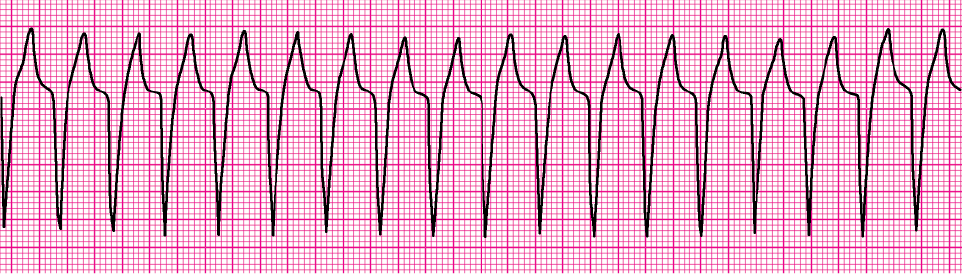
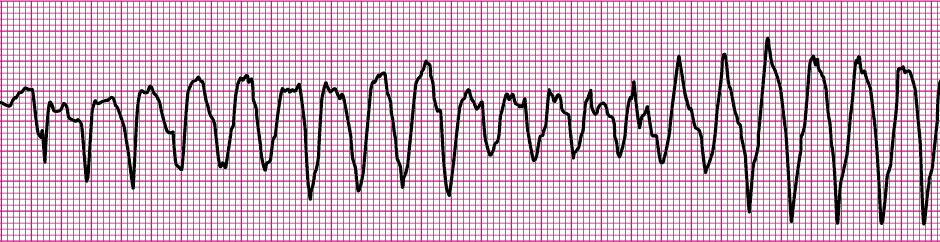
Clinical clue: heart rate 214/min.
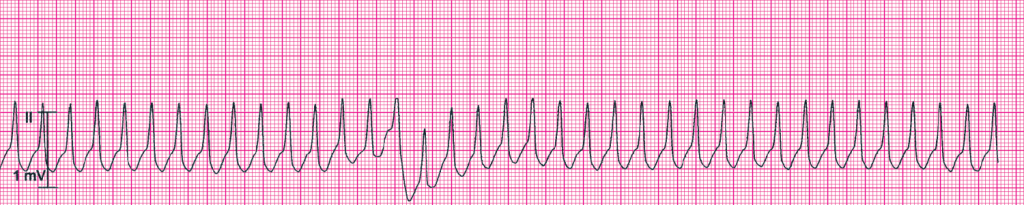
Answer: Wide complex tachycardia.
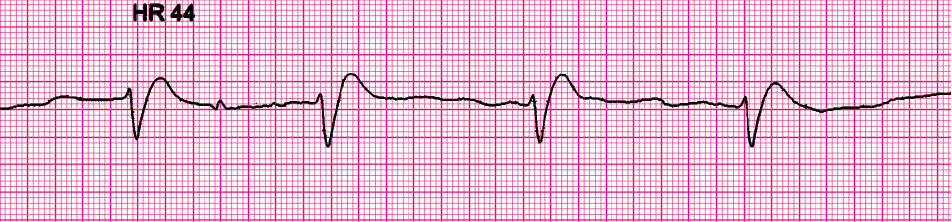
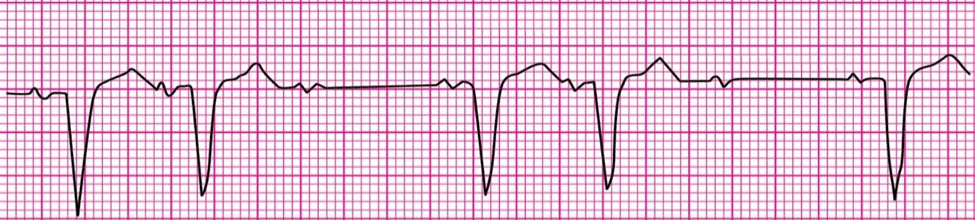
Clinical clues: age 7 years; heart rate 38/min.
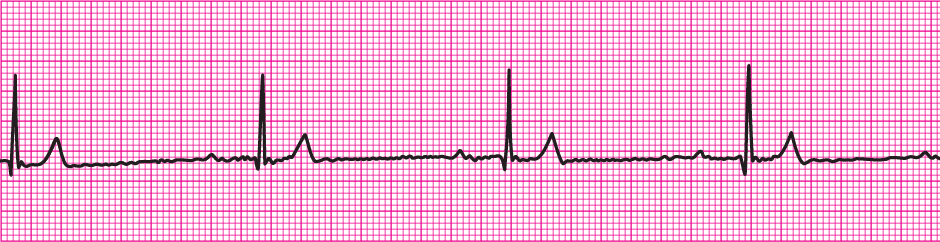
Answer: Sinus bradycardia.
Clinical clues: initial rhythm associated with heart rate 300/min.

Answer: SVT converting to sinus rhythm after adenosine administration.
Clinical clues: heart rate 150/min.
Answer: Wide complex tachycardia.
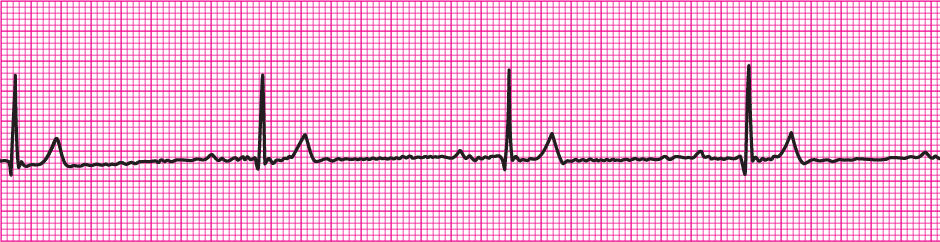
Clinical clues: age 8 years; heart rate 78/min.
Answer: Normal sinus rhythm.
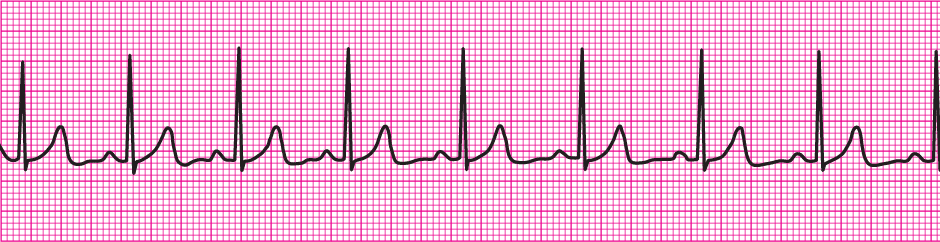
Clinical clues: febrile infant; heart rate 188/min.

Answer: Sinus tachycardia.
Clinical clues: age 3 months; heart rate 65/min.

Answer: Sinus bradycardia.
Clinical clues: heart rate 200/min; no detectable pulses.
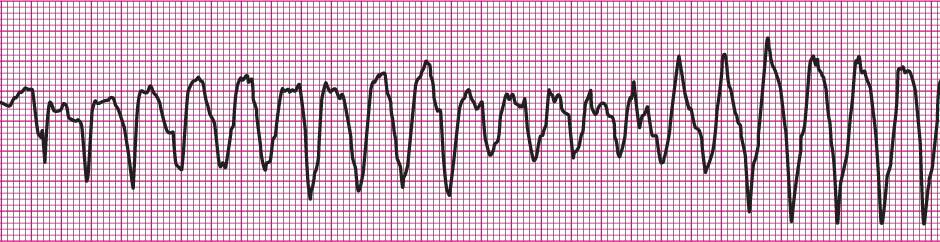
Answer: Torsades de pointed.
Clinical clue: no detectable pulses.

Answer: Asystole.
Clinical clues: initial rhythm associated with no detectable pulses.

Answer: VF with successful defib and resumption of organized rhythm.
Clinical clues: no consistent heart rate detected; no detectable pulses.

Answer: Ventricullar fibrillation.
Clinical clue: heart rate 300/min.

Answer: Supraventricular tachycardia (SVT).
Section 2: Pharmacology Answers
A 9-year-old boy is agitated and leaning forward on the bed in obvious respiratory distress. The patient is speaking in short phrases and tells you that he has asthma but does not carry an inhaler. He has nasal flaring, severe suprasternal and intercostal retractions, and decreased air movement with prolonged expiratory time and wheezing. You administer 100% oxygen by a nonrebreathing mask. His SpO2 is 92%. Which medication do you prepare to give to this patient?
A. Adenosine
B. Procainamide
C. Amiodarone
D. Albuterol (Correct)
Which oxygen delivery system most reliably delivers a high (90% or greater) concentration of inspired oxygen to a 7-year-old child?
A. Face tent
B. Simple oxygen mask
C. Nonrebreathing face mask (Correct)
D. Nasal cannula
You are part of a team attempting to resuscitate a child with ventricular fibrillation cardiac arrest. You delivered 2 unsynchronized shocks. A team member established IO access, so you give a dose of epinephrine, 0.01 mg/kg IO. At the next rhythm check, persistent ventricular fibrillation is present. You administer a 4-J/kg shock and resume CPR. Which drug and dose should be administered next?
A. Magnesium sulfate 25 to 50 mg/kg IO
B. Epinephrine 0.1 mg/kg IO
C. Atropine 0.02 mg/kg IO
D. Amiodarone 5 mg/kg IO (Correct)
Which statement is correct about the effects of epinephrine during attempted resuscitation?
A. Epinephrine decreases myocardial oxygen consumption
B. Epinephrine is contraindicated in ventricular fibrillation
C. Epinephrine stimulates spontaneous contractions when asystole is present (Correct)
D. Epinephrine decreases peripheral vascular resistance and reduces myocardial afterload
You are called to help treat an infant with severe symptomatic bradycardia (heart rate 66/min) associated with respiratory distress. The bradycardia persists despite establishment of an effective airway, oxygenation, and ventilation. There is no heart block present. Which is the first drug you should administer?
A. Atropine
B. Dopamine
C. Adenosine
D. Epinephrine (Correct)
Which statement is correct about endotracheal drug administration during resuscitative efforts for pediatric patients?
A. The intravenous drug dose should be used
B. It is the preferred route of drug administration
C. It is the least desirable route of administration (Correct)
D. The drug dose used is lower than the intravenous dose
Which statement is correct about the use of calcium chloride in pediatric patients?
A. It has the same bioavailability of elemental calcium as calcium gluconate
B. The recommended dose is 1 to 2 mg/kg
C. Routine administration is not indicated during cardiac arrest (Correct)
D. It is indicated for hypercalcemia, hypokalemia, and hypomagnesemia
A previously healthy infant with a history of vomiting and diarrhea is brought to the emergency department by her parents. During your assessment, you find that the infant responds only to painful stimulation. The infant’s respiratory rate is 40 breaths per minute, and central pulses are rapid and weak. The infant has good bilateral breath sounds, cool extremities, and a capillary refill time of more than 5 seconds. The infant’s blood pressure is 85/65 mm Hg, and glucose is 30 mg/dL (1.65 mmol/L). You administer 100% oxygen via face mask and start an IV. Which treatment is the most appropriate for this infant?
A. Administer a bolus of isotonic crystalloid 20 mL/kg over 5 to 20 minutes, and also give D25W 2 to 4 mL/kg IV (Correct)
B. Administer lactated Ringer’s solution 20 mL/kg over 60 minutes
C. Administer D50W 0.45% sodium chloride 20 mL/kg bolus over 15 minutes
D. Administer D10W 20 mL/kg bolus over 5 minutes
Initial impression of a 2-year-old girl shows her to be alert with mild breathing difficulty during inspiration and pale skin color. On primary assessment, she makes high-pitched inspiratory sounds (mild stridor) when agitated; otherwise, her breathing is quiet. Her SpO2 is 92% on room air, and she has mild inspiratory intercostal retractions. Lung auscultation reveals transmitted upper airway sounds with adequate distal breath sounds bilaterally. Which is the most appropriate initial intervention for this child?
A. IV dexamethasone
B. Humidified oxygen as tolerated (Correct)
C. Nebulized albuterol
D. Endotracheal intubation
Paramedics are called to the home of a 1-year-old child. Their initial assessment reveals a child who responds only to painful stimuli and has irregular breathing, faint central pulses, bruises over the abdomen, abdominal distention, and cyanosis. Bag-mask ventilation with 100% oxygen is initiated. The child’s heart rate is 36/min. Peripheral pulses cannot be palpated, and central pulses are barely palpable. The cardiac monitor shows sinus bradycardia. Two-rescuer CPR is started. Upon arrival to the emergency department, the child is intubated and ventilated with 100% oxygen, and IV access is established. The heart rate is now 150/min with weak central pulses but no distal pulses. Systolic blood pressure is 74 mm Hg. Which intervention should be provided next?
A. Rapid bolus of 20 mL/kg of isotonic crystalloid (Correct)
B. Amiodarone 5 mg/kg IV
C. Atropine 0.02 mg/kg IV
D. Epinephrine 0.01 mg/kg IV
Section 3: Practical Application Answers
You need to provide rescue breaths to a child victim with a pulse. What is the appropriate rate for delivering breaths?
A. 1 breath every 6 seconds
B. 1 breath every 3 to 5 seconds
C. 2 breaths every 6 to 8 seconds
D. 1 breath every 2 to 3 seconds (Correct)
A 3-year-old unresponsive, apneic child is brought to the emergency department. EMS personnel report that the child became unresponsive as they arrived at the hospital. The child is receiving CPR with bag-mask ventilation. The rhythm shown here is on the cardiac monitor. A biphasic manual defibrillator is present. You quickly use the length from head to heel of the child on a color-coded length-based resuscitation tape to estimate the approximate weight as 15 kg. Which therapy is most appropriate for this child at this time?

A. Attempt defibrillation at 10 J, and then resume CPR, beginning with compressions
B. Attempt defibrillation at 30 J, and then open the airway and check for a pulse
C. Attempt defibrillation at 30 J, and then resume CPR, beginning with compressions (Correct)
D. Establish IV/IO access and administer epinephrine 0.01 mg/kg IV/IO
You are supervising a student who is inserting an IO needle into an infant’s tibia. The student asks you what she should look for to know that she has successfully inserted the needle into the bone marrow cavity. What do you tell her?
A. “Once inserted, the shaft of the needle moves easily in all directions within the bone.”
B. “Proper placement will always yield blood return.”
C. “Pulsatile blood flow will be present in the needle hub.”
D. “Fluids can be administered freely without local soft tissue swelling.” (Correct)
A 4-year-old boy is in pulseless arrest in the pediatric intensive care unit. High-quality CPR is in progress. You quickly review his chart and find that his baseline-corrected QT interval on a 12-lead ECG is prolonged. The monitor shows recurrent episodes of the rhythm shown here. The patient has received 1 dose of epinephrine 0.01 mg/kg, but the rhythm shown here continues. If this rhythm persists at the next rhythm check, which medication would be most appropriate to administer at that time?
A. Epinephrine 0.1 mg/kg IV
B. Lidocaine 1 mg/kg IV
C. Adenosine 0.1 mg/kg IV
D. Magnesium sulfate 25 to 50 mg/kg IV (Correct)
You are caring for a 3-year-old with vomiting and diarrhea. You have established IV access. The child’s pulses are palpable but faint, and the child is now lethargic. The heart rate is variable (range, 44/min to 62/min). You begin bag-mask ventilation with 100% oxygen. When the heart rate does not improve, you begin chest compressions. The rhythm shown here is seen on the cardiac monitor. Which would be the most appropriate therapy to consider next?
A. Atropine 0.02 mg/kg IV (Correct)
B. Epinephrine 0.1 mg/kg IV
C. Transcutaneous pacing
D. Synchronized cardioversion at 0.5 J/kg
What ratio of compressions to breaths should be used for 1-rescuer child CPR?
A. 100 to 120 compressions per minute with no breaths
B. 30 compressions to 2 breaths (Correct)
C. 15 compressions to 2 breaths
D. 50 compressions to 1 breath
A pale and very sleepy but arousable 3-year-old child with a history of diarrhea is brought to the hospital. Primary assessment reveals a respiratory rate of 45/min with good breath sounds bilaterally. Heart rate is 150/min, blood pressure is 90/64 mm Hg, and SpO2 is 92% in room air. Capillary refill is 5 seconds, and peripheral pulses are weak. After placing the child on a nonrebreathing face mask (10-L/min flow) with 100% oxygen and obtaining vascular access, which is the most appropriate immediate treatment for this child?
A. Administer a dopamine infusion at 2 to 5 mcg/kg per minute
B. Begin a maintenance crystalloid infusion
C. Obtain a chest x-ray
D. Administer a bolus of 20 mL/kg isotonic crystalloid (Correct)
How can rescuers ensure that they are providing effective breaths when using a bag-mask device?
A. By delivering breaths quickly and forcefully
B. By observing the chest rise with each breath (Correct)
C. By allowing air to release around the mask
D. By always having oxygen attached to the bag
You are giving chest compressions for a child in cardiac arrest. What is the proper depth of compressions for a child?
A. Compress the chest at least one third the depth of the chest, approximately 2 inches (5 cm) (Correct)
B. Compress the chest at least one fourth the depth of the chest, approximately 1.5 inches (4 cm)
C. Compress the chest at least two thirds the depth of the chest, approximately 4 inches (10 cm)
D. Compress the chest at least one half the depth of the chest, approximately 3 inches (8 cm)
You find an infant who is unresponsive, is not breathing, and does not have a pulse. You shout for nearby help, but no one arrives. What action should you take next?
A. Provide CPR for 60 seconds before leaving to activate the emergency response system
B. Activate the emergency response system after giving CPR for 90 seconds
C. Provide CPR for approximately 2 minutes before leaving to activate the emergency response system (Correct)
D. Activate the emergency response system after giving CPR for 10 minutes
You and another rescuer begin CPR. Your colleague begins compressions, and you notice that the compression rate is too slow. What should you say to offer constructive feedback?
A. “You need to compress at a rate of 100 to 120 per minute.” (Correct)
B. “You need to compress at a rate of at least 100 per minute.”
C. “You need to compress at a rate of at least 120 per minute.”
D. “You need to compress at a rate of 80 to 120 per minute.”
A child becomes unresponsive in the emergency department and is not breathing. You are uncertain if a faint pulse is present. You shout for help and provide ventilation with 100% oxygen. The rhythm shown here is seen on the cardiac monitor. What is your next action?

A. Establish IV access and give epinephrine 0.01 mg/kg IV
B. Prepare for transcutaneous pacing
C. Establish IV access and give atropine 0.01 mg/kg IV
D. Start high-quality CPR (Correct)
An 8-month-old infant is brought to the emergency department for evaluation of severe diarrhea and dehydration. On arrival to the emergency department, the infant becomes unresponsive, apneic, and pulseless. You shout for help and start CPR. Another provider arrives, at which point you switch to 2-rescuer CPR. The rhythm shown here is seen on the cardiac monitor. The infant is intubated and ventilated with 100% oxygen. An IO line is established, and a dose of epinephrine is given. While continuing high-quality CPR, what do you do next?
A. Give atropine 0.02 mg/kg IO
B. Give amiodarone 5 mg/kg IO
C. Give normal saline 20 mL/kg IO rapidly (Correct)
D. Give epinephrine 0.1 mg/kg IO
A 3-year-old boy presents with multiple-system trauma. The child was an unrestrained passenger in a high-speed motor vehicle crash. On primary assessment, he is unresponsive to voice or painful stimulation. His respiratory rate is 5/min, heart rate and pulses are 170/min, systolic blood pressure is 60 mm Hg, capillary refill is 5 seconds, and SpO2 is 75% on room air. Which action should you take first?
A. Establish immediate vascular access
B. Provide 100% oxygen by simple mask
C. While a colleague provides spinal motion restriction, open the airway with a jaw thrust and provide bag-mask ventilation (Correct)
D. Perform immediate endotracheal intubation
A 7-year-old boy is found unresponsive, apneic, and pulseless. CPR is ongoing. The child is intubated, and vascular access is established. The ECG monitor shows an organized rhythm with a heart rate of 45/min, but a pulse check reveals no palpable pulses. High-quality CPR is resumed, and an initial IV dose of epinephrine is administered. Which intervention should you perform next?
A. Perform defibrillation
B. Perform synchronized cardioversion
C. Administer epinephrine
D. Identify and treat reversible causes (Correct)
You are preparing to use a manual defibrillator in the pediatric setting. Which best describes when it is appropriate to use the smaller, pediatric-sized paddles?
A. If the child weights less than 40 kg or is less than 10 years old
B. If the child weights less than 20 kg or is less than 3 years old
C. If the child weights less than 30 kg or is less than 5 years old
D. If the child weighs less than 10 kg or is less than 1 year old (Correct)
During bag-mask ventilation, how should you hold the mask to make an effective seal between the child’s face and the mask?
A. Push the jaw forward by using a jaw-thrust maneuver
B. Position your fingers using the E-C clamp technique (Correct)
C. Position your fingers using the bridge of the nose as a guide
D. Use the 2 thumb‒encircling hands technique
An 18-month-old child has a 1-week history of cough and runny nose. The child has diffuse cyanosis and is responsive only to painful stimulation with slow respirations and rapid central pulses. The child’s respiratory rate has decreased from 65/min to 10/min, severe inspiratory intercostal retractions are present, heart rate is 160/min, SpO2 is 65% in room air, and capillary refill is less than 2 seconds. Which are the most appropriate immediate interventions for this toddler?
A. Administer 100% oxygen by face mask, obtain an arterial blood gas, and establish vascular access
B. Administer 100% oxygen by face mask, establish vascular access, and obtain a chest x-ray stat
C. Open the airway and provide positive-pressure ventilation using 100% oxygen and a bag-mask device (Correct)
D. Establish vascular access and administer a 20 mL/kg bolus of isotonic crystalloid
An 8-year-old child was struck by a car. He arrives in the emergency department alert, anxious, and in respiratory distress. His cervical spine is immobilized, and he is receiving a 10-L/min flow of 100% oxygen by nonrebreathing face mask. His respiratory rate is 60/min, heart rate 150/min, systolic blood pressure 70 mm Hg, and SpO2 84%. Breath sounds are absent over the right chest but present over the left chest, and the trachea is deviated to the left. He has weak central pulses and absent distal pulses. Which intervention should be performed next?
A. Perform needle decompression of the right chest (Correct)
B. Provide bag-mask ventilation
C. Establish IV access
D. Perform endotracheal intubation
What compression-to-ventilation ratio should be used for 2-rescuer infant CPR?
A. 15 compressions to 2 breaths (Correct)
B. 5 compressions to 1 breath
C. 20 compressions to 2 breaths
D. 30 compressions to 2 breaths
You just assisted with the elective endotracheal intubation of a child with respiratory failure and a perfusing rhythm. Which provides a reliable, prompt assessment of correct endotracheal tube placement in this child?
A. Adequate bilateral breath sounds and chest expansion plus detection of ETCO2 with waveform capnography (Correct)
B. Absence of audible breath sounds over the abdomen during positive-pressure ventilation
C. Confirmation of appropriate oxygen and carbon dioxide tensions on arterial blood gas analysis
D. Auscultation of breath sounds over the lateral chest bilaterally plus presence of mist in the endotracheal tube
A 10-month-old infant boy is brought to the emergency department. Your initial assessment reveals a lethargic, pale infant with slow respirations and slow, weak central pulses. One team member begins ventilation with a bag-mask device with 100% oxygen. A second team member attaches the monitor/defibrillator and obtains vital signs while a third team member attempts to establish IV/IO access. The patient’s heart rate is 38/min with the rhythm shown here. The infant’s blood pressure is 58/38 mm Hg, and capillary refill is 4 seconds. His central pulses remain weak, and distal pulses cannot be palpated. Chest compressions are started and IO access is obtained. Which medication do you anticipate will be given next?
A. Atropine 0.02 mg/kg IV/IO
B. Epinephrine 0.01 mg/kg IV/IO (Correct)
C. Epinephrine 0.1 mg/kg IV/IO
D. Adenosine 0.1 mg/kg rapid IV/IO
A 1-year-old boy is brought to the emergency department for evaluation of poor feeding, irritability, and sweating. The child is lethargic but arousable. He has labored breathing, very rapid pulses, and a dusky color. His respiratory rate is 68/min, heart rate 300/min, and blood pressure 70/45 mm Hg. He has weak brachial pulses and absent radial pulses, a capillary refill of 6 seconds, SpO2 85% in room air, and good bilateral breath sounds. You administer high-flow oxygen and place the child on a cardiac monitor and see the rhythm shown here. The child has no history of congenital heart disease. IV access has been established. Which therapy is most appropriate for this child?

A. Administer isotonic crystalloid fluid bolus of 20 mL/kg
B. Consult with pediatric cardiology
C. Perform immediate defibrillation
D. Administer adenosine 0.1 mg/kg IV rapid push (Correct)
You are evaluating an irritable 6-year-old girl with mottled skin color. The patient is febrile (temperature 40°C [104°F]), and her extremities are cold with capillary refill of 5 seconds. Distal pulses are absent and central pulses are weak. Heart rate is 180/min, respiratory rate is 45/min, and blood pressure is 98/56 mm Hg. How would you categorize this child’s condition?
A. Hypotensive shock associated with inadequate tissue perfusion
B. Compensated shock associated with tachycardia and inadequate tissue perfusion (Correct)
C. Hypotensive shock associated with inadequate tissue perfusion and significant hypotension
D. Compensated shock requiring no intervention
You find a 10-year-old boy to be unresponsive. You shout for help, and after finding that he is not breathing and has no pulse, you and a colleague begin CPR. Another colleague activates the emergency response system, brings the emergency equipment, and places the child on a cardiac monitor/defibrillator, which reveals the rhythm shown here. You attempt defibrillation at 2 J/kg and give 2 minutes of CPR. The rhythm persists at the second rhythm check, at which point you attempt defibrillation with 4 J/kg. A fourth colleague arrives, starts an IV, and administers 1 dose of epinephrine 0.01 mg/kg. If ventricular fibrillation or pulseless ventricular tachycardia persists after 2 minutes of CPR, you will administer another shock. Which drug and dose should be administered next?

A. Atropine 0.02 mg/kg IV
B. Lidocaine 1 mg/kg IV (Correct)
C. Adenosine 0.1 mg/kg IV
D. Epinephrine 0.1 mg/kg IV
Why is allowing complete chest recoil important when performing high-quality CPR?
A. The heart will refill with blood between compressions (Correct)
B. It will reduce the risk of rib fractures
C. The rate of chest compressions will increase
D. There will be a reduction in rescuer fatigue
You are assisting in the elective intubation of an average-sized 4-year-old child with respiratory failure. A colleague is retrieving the color-coded length-based tape from the resuscitation cart. Which of the following is likely to be the estimated size of the uncuffed endotracheal tube for this child?
A. 4-mm tube
B. 6-mm tube
C. 5-mm tube (Correct)
D. 3-mm tube
You are alone and witness a child suddenly collapse. There is no suspected head or neck injury. A colleague responded to your shout for help and is activating the emergency response system and is retrieving the resuscitation equipment, including a defibrillator. After delivering 30 compressions, what would be your next action?
A. Use a bag-mask device to deliver 6 breaths per minute
B. Check for a carotid pulse for no more than 10 seconds
C. Open the airway with a head tilt‒chin lift maneuver and give 2 breaths (Correct)
D. Assess for lack of breathing or only gasping for 10 seconds
You are caring for a 6-year-old patient who is receiving positive-pressure mechanical ventilation via an endotracheal tube. The child begins to move his head and suddenly becomes cyanotic, and his heart rate decreases. His SpO2 is 65%. You remove the child from the mechanical ventilator and begin to provide manual ventilation with a bag via the endotracheal tube. During manual ventilation with 100% oxygen, the child’s color and heart rate improve slightly and his blood pressure remains adequate. Breath sounds and chest expansion are present and adequate on the right side and are present but consistently diminished on the left side. The trachea is not deviated, and the neck veins are not distended. A suction catheter passes easily beyond the tip of the endotracheal tube. Which of the following is the most likely cause of this child’s acute deterioration?
A. Tension pneumothorax on the right side
B. Equipment failure
C. Tracheal tube displacement into the right main bronchus (Correct)
D. Tracheal tube obstruction