Basic A 35 Questions
Read Also: Relias Dysrhythmia Basic B Test Answers.
Study Set

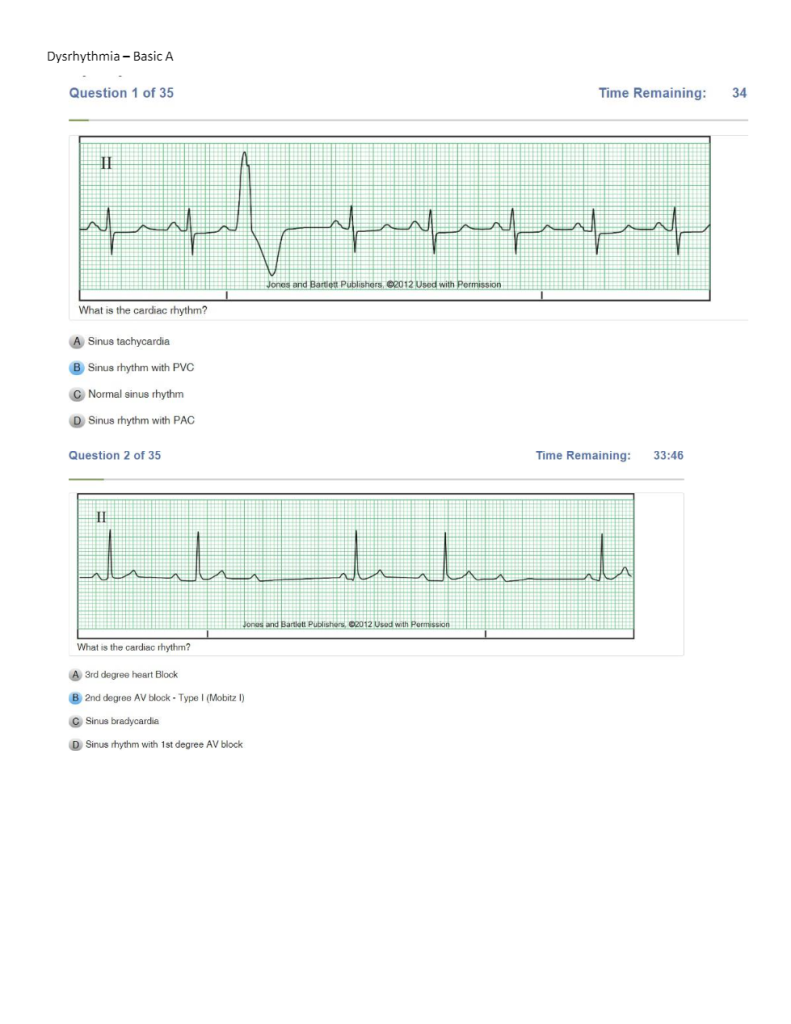
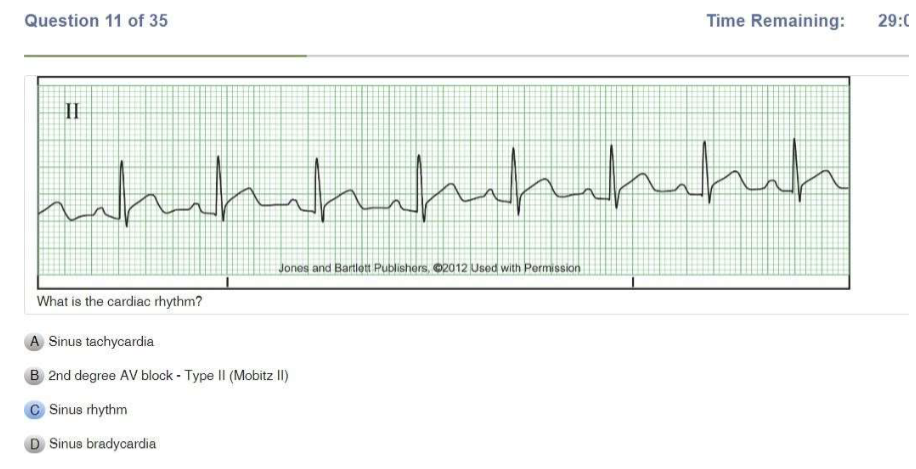
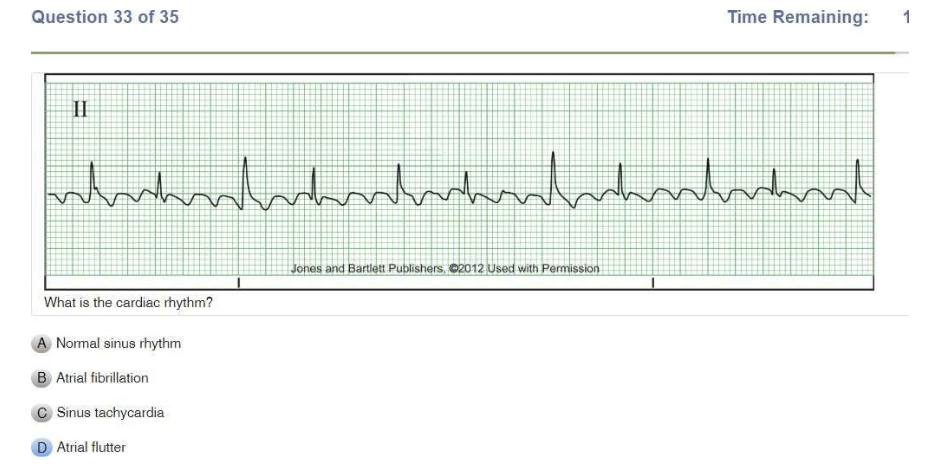
| Normal sinus rhythm | Regular Rate: 60-100 P Wave: Present, upright PR Interval: 0.12-0.20 sec QRS: <0.12 sec |
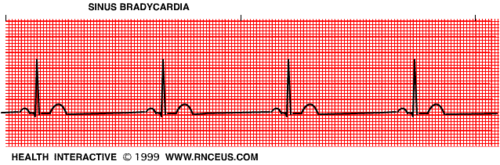
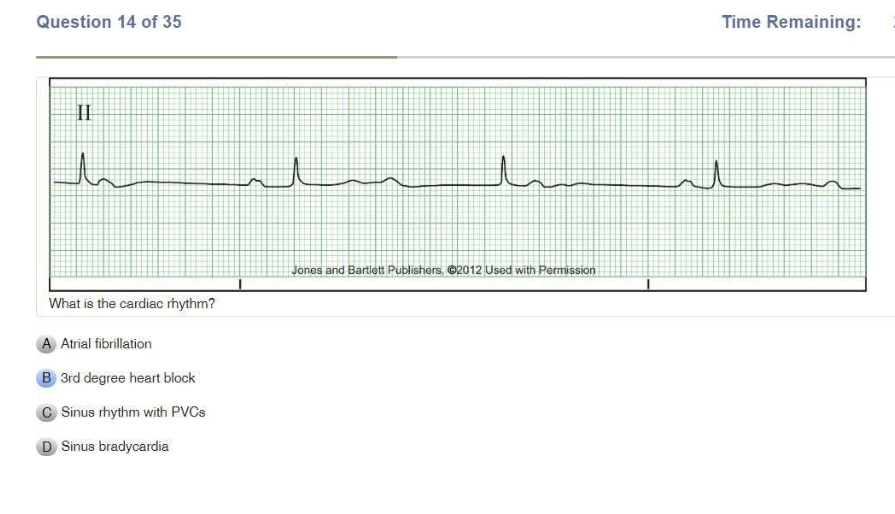
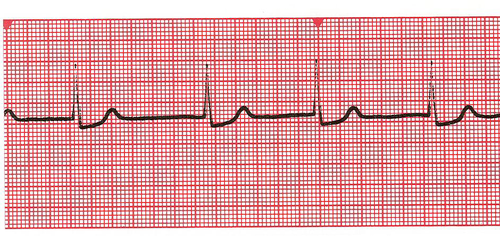
| Sinus Bradycardia | Regular Rate: <60 P Wave: Present, upright PR Interval: 0.12-0.20 sec QRS: <0.12 sec |
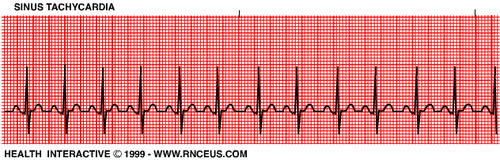
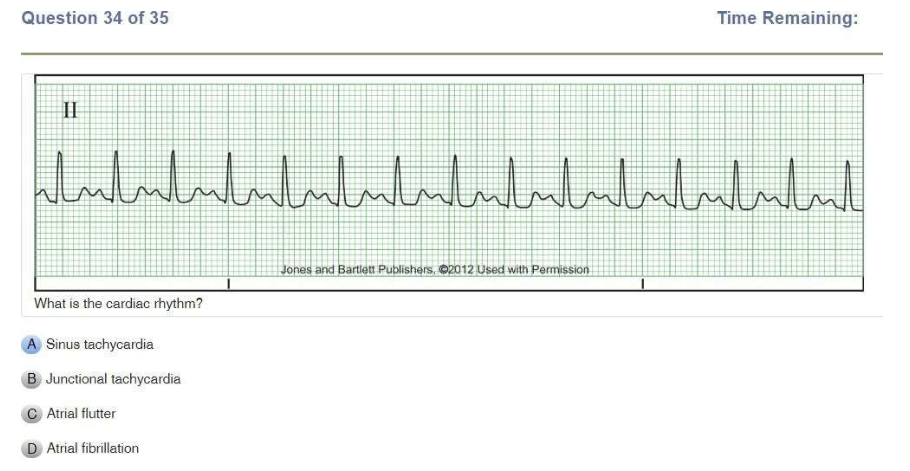
| Sinus Tachycardia | Regular Rate: 100-150 P Wave: Present, upright PR Interval: 0.12-0.20 sec QRS: <0.12 sec |
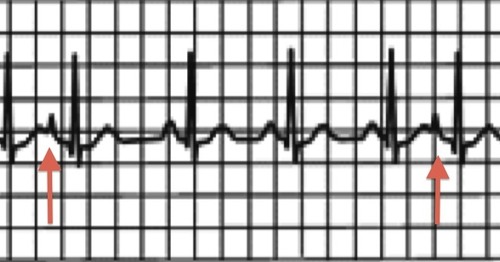
| Premature Atrial Contraction | IRREGULAR Rate: depends on underlying rhythm P wave: Present or hidden in T wave PR Interval: 0.12-0.20 sec QRS: <0.12 sec |
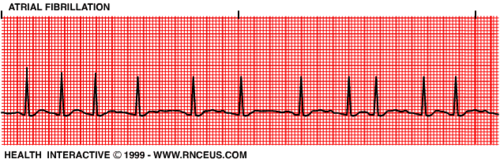
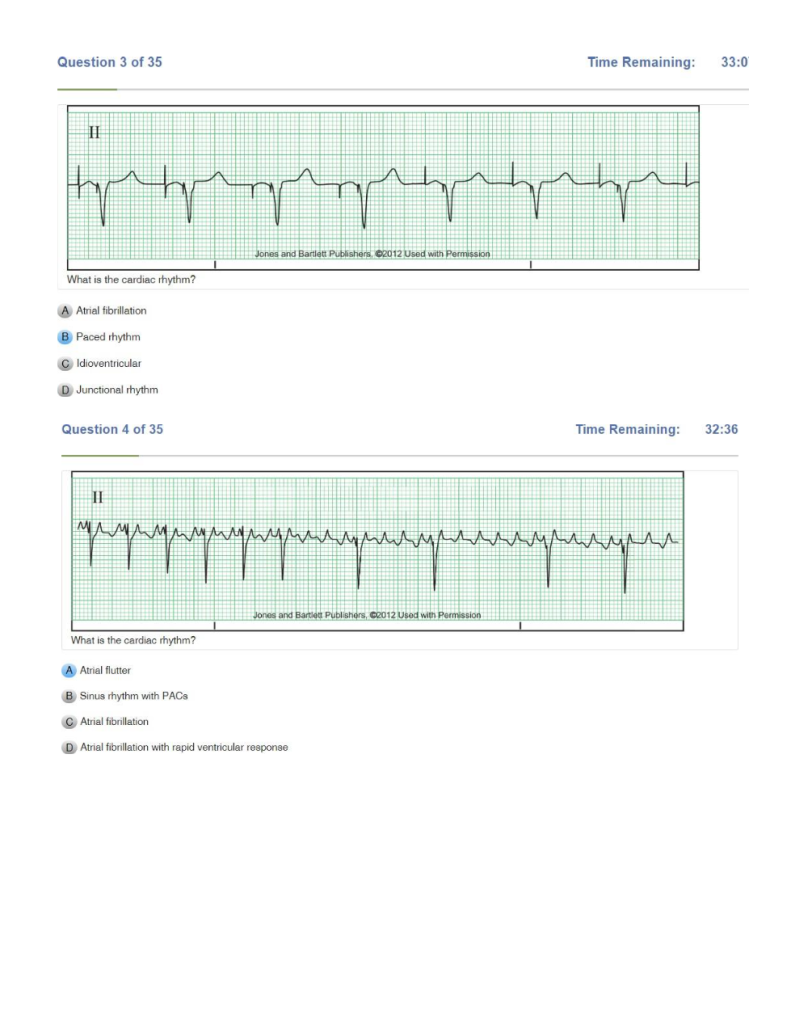
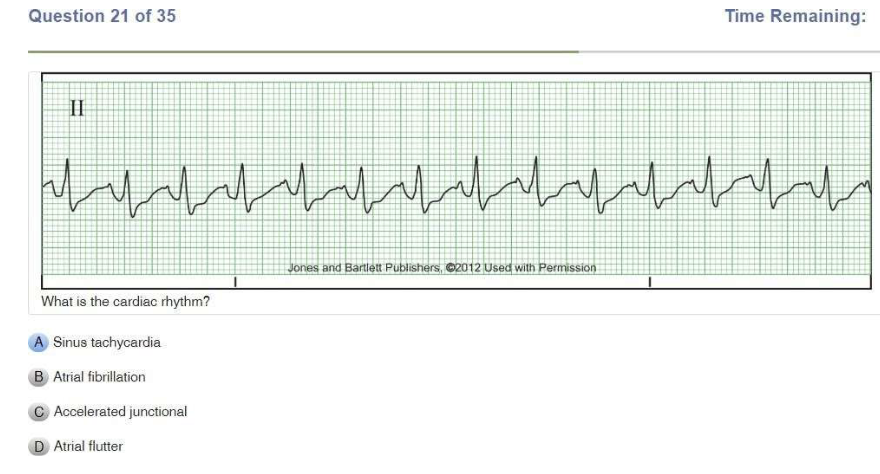
| Atrial Fibrillation | IRREGULAR Atrial rate: UNMEASURABLE Ventricular rate: variable P wave: unable to see PR Interval: N/A QRS: <0.12 sec |
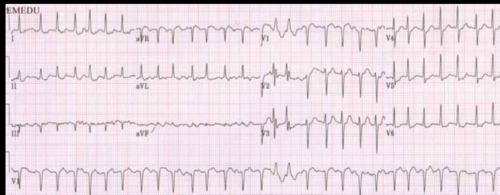
| A fib RVR | IRREGULAR Ventricular rate: 100-175 P wave: unable to see PR Interval: N/A QRS <0.12 sec |

| Atrial Flutter | Usually REGULAR can be irregular Atrial rate: 250-350 Ventricular rate: variable BUT < atrial rate P Wave: Flutter PR Interval: N/A QRS: <0.12 sec |

| Supraventricular Tachycardia | Regular Rate: 150-350 P wave: Hidden in QRS or T wave PR: unable to determine QRS: <0.12 sec |
| Junctional Rhythm | Regular Rate: 40-60 P Wave: ABSENT or INVERTED PR Interval: None or <0.12 QRS: <0.12 sec |

| Accelerated Junctional Rhythm | Regular Rate: 60-100 P Wave: NONE or INVERTED PR Interval: None or <0.12 QRS: <0.12 sec |
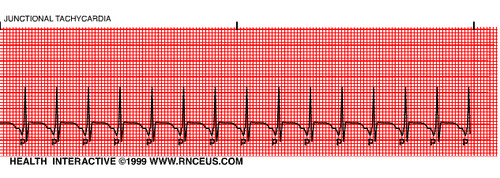
| Junctional Tachycardia | Regular Rate: >100 P Wave: NONE or INVERTED PR Interval: None or <0.12 QRS: <0.12 sec |
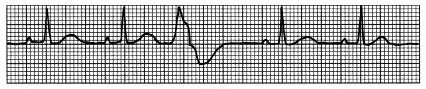
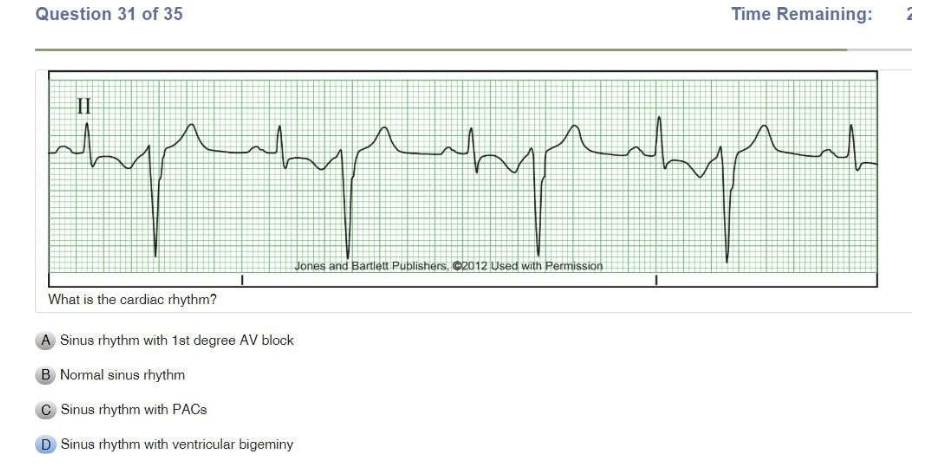
| Premature Ventricular Contraction | IRREGULAR Rate: refer to underlying rhythm P Wave: NONE PR Interval: N/A QRS: WIDE and BIZARRE , >0.12 sec |
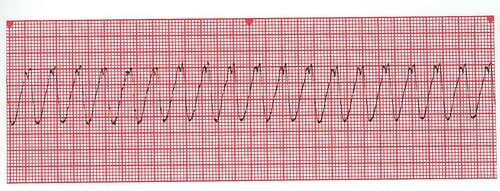
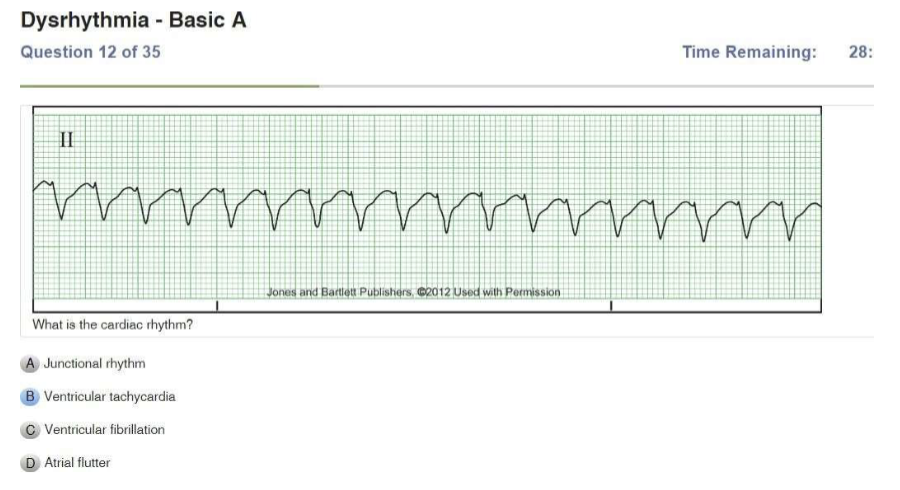
| Ventricular Tachycardia | Regular Rate: >100 P Wave: NONE PR Interval: N/A QRS: WIDE and BIZARRE, >0.12 sec |

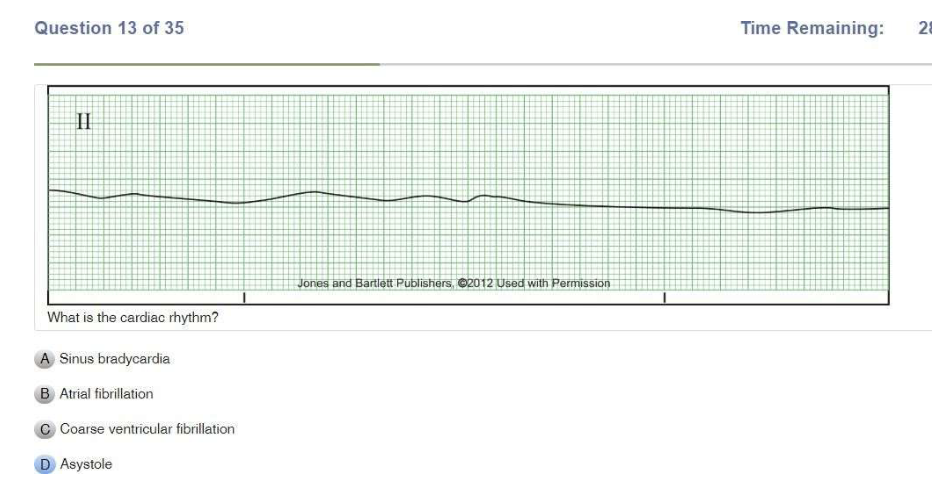
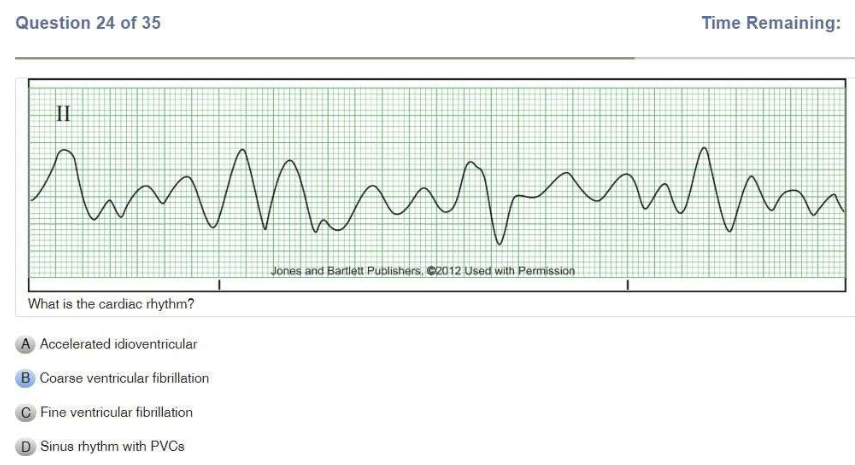
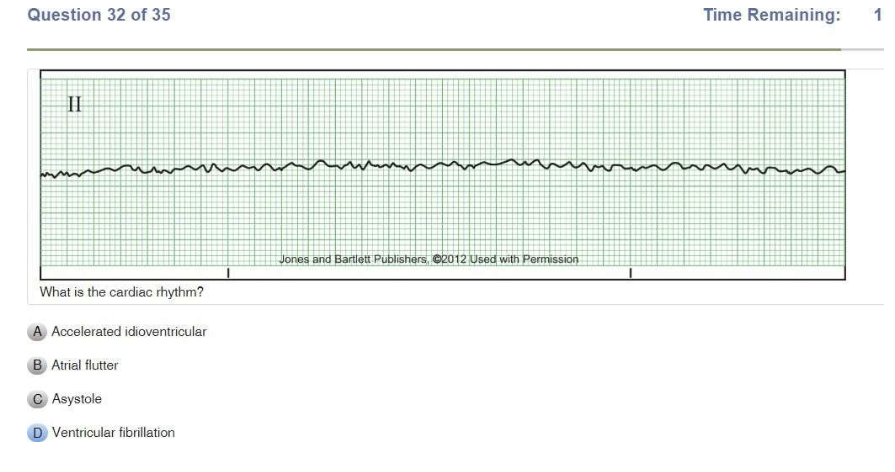
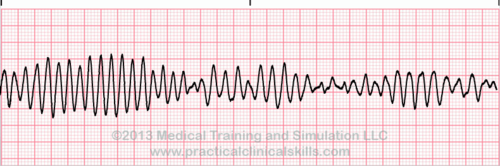
| Ventricular Fibrillation | Chaotic Coarse: big waves Fine: small waves Rate: unmeasurable P Wave: NONE PR Interval: N/A QRS: N/A |

| Idioventricular | Regular Rate: 20-50 P wave: NONE PR Interval: N/A QRS: WIDE, >0.12 sec |

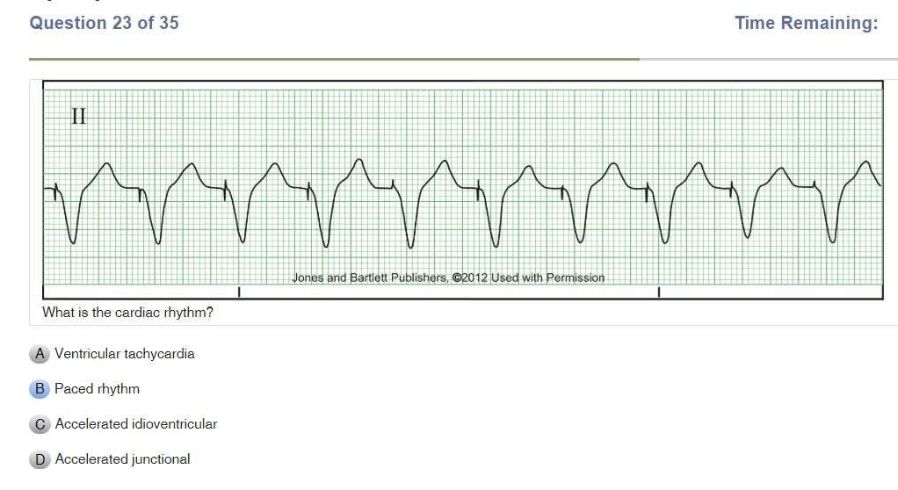
| Accelerated Idoventricular Rhythm | Regular Rate: 50-100 P wave: NONE PR Interval: N/A QRS: WIDE, >0.12 sec |
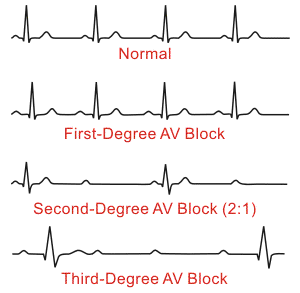
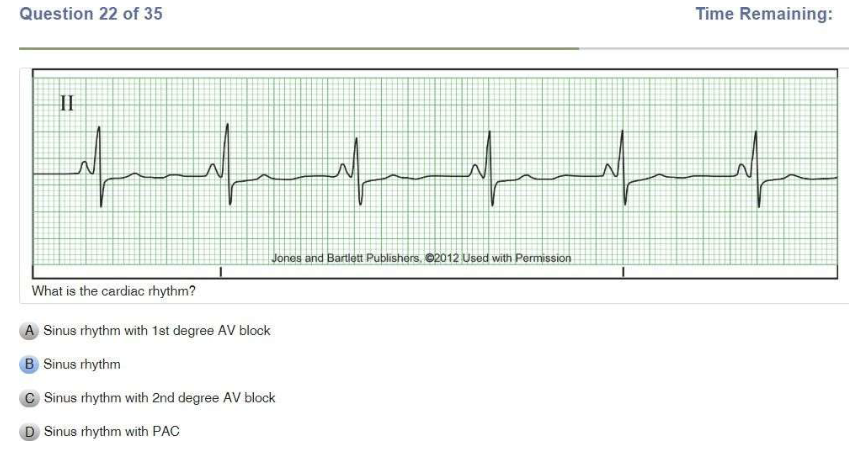
| 1st Degree AV Block | Regular Rate: 60-100 P Wave: Present, upright PR interval: >0.20 sec CONSISTENTLY LONG QRS: <0.12 sec Husband stays late till 9 consistently |

| 2nd Degree AV Block Type I Mobitz, Wenckebach | IRREGULAR Rate: 60-100 P wave: Present, upright PR Interval: Progressively longer until drop (PR interval longer and longer until drop) QRS: <0.12 sec Husband stays late till 9, then 11, then 1, then doesn’t come home at all |
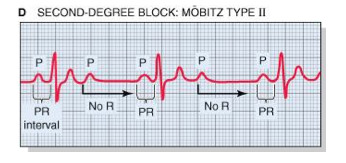
| 2nd Degree AV Block Type II | Irregular or regular Rate: <60 P wave: Present, upright PR Interval: PR interval consistently LONGER like type 1 but then a QRS will drop QRS: <0.12 sec Husband stays late till 9 consistently, then wife goes out and doesn’t come home |
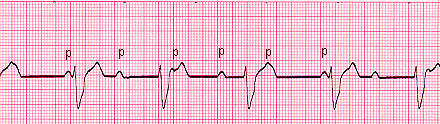
| 3rd Degree AV Block | Atrials and ventricles don’t communicate Rate: regular atrial P wave: Present, upright No relationship between P waves and QRS PR Interval: VARIABLE QRS: variable P-P ad R-R consistent but NO correlation Husband and wife live separate lives and don’t communicate |
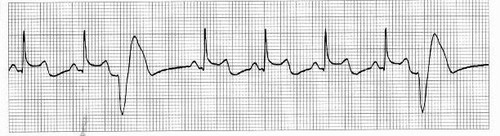
| Unifocal PVCs | Only 1 shape PVC |

| Monomorphic V Tach | Same Shapes V Tach |
| Polymorphic V Tach | Different Shapes V tach |

| Coarse V Fib | Chopy but not as high as polymorphic V tach |
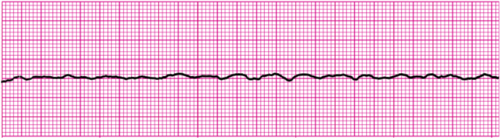
| Fine V Fib | Fine and fibrillatory |

| Failure to Capture | Spikes with no QRS |
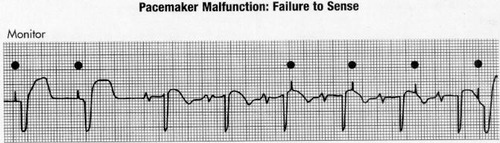
| Failure to Sense | Spikes happen regardless of QRS on their own |
Cardiac Conduction System Rates
| Component | Order | Rate (beats per minute) |
|---|---|---|
| SA Node | 1st | 60-100 |
| AV Node | 2nd | 40-60 |
| Bundle of His | 3rd | 40-45 |
| Right and Left Bundle Branches | 4th | 40-45 |
| Purkinje Fibers | 5th | 20-50 |
ECG Box Measurements
| Description | Measurement |
|---|---|
| 1 Small Box | 0.04 sec |
| 1 Big Box | 0.20 sec |
Junctional Rhythms Characteristics
| Feature | Description |
|---|---|
| SA Node Status | DID NOT FIRE |
| AV Node Status | Fired |
| P Wave | NO P WAVE bc SA node didn’t fire |
| QRS Complex | Narrow QRS |
Wave Measurements
| Wave | Characteristic | Measurement |
|---|---|---|
| P Wave | Amplitude; Compared to T wave; Origin | 0.5-2.5 mm; Will be shorter than T wave; Shows firing of SA node |
| QRS | Duration; Criteria; Implications | 0.06-0.10 sec SHOULD BE <0.12 sec; Wide QRS indicates delay in ventricular contraction or conduction delay through bundle branches or Purkinje fibers; BUNDLE BRANCH BLOCK or BLOCK IN PURKINJE FIBERS (idioventricular) |
Heart Rate Calculation Methods
| Method | Formula |
|---|---|
| Calculate Regular Rate | 1500 / # boxes between R-R |
| Calculate Irregular Rate | # of Rs in 6 sec strip X 10 |
Types of PVC Arrhythmias
| Arrhythmia | Description |
|---|---|
| Bigeminy | PVC occurs every OTHER beat |
| Trigeminy | PVC occurs every THIRD beat |
| Couplet | 2 PVCs together |
| Triplet | 3 PVCs together |
| Multifocal | Multiple shapes |
Was this helpful?
Let us know if this was helpful. That’s the only way we can improve.